


President’s Letter
2023 Metrics
Cycle of Translation
Visionary Gifts
Discovery to Clinic
Innovative Education
Translational Luminaries
Introduction
Jerold B. Katz Academy of Translational Research
Infectious Diseases Research Fund
Houston Methodist Dr. Mary and Ron Neal Cancer Center
Ann Kimball and John W. Johnson Center for Cellular Therapeutics at Houston Methodist
The Food & Health Alliance within the Houston Methodist Lynda K. and David M. Underwood Center for Digestive Disorders, Immunology Center and the Fondren Inflammation Collaborative
Houston Methodist Cockrell Center for Advanced Therapeutics
Paula and Joseph C. “Rusty” Walter III
Translational Research Initiative

COVID-19 Studies
Outcomes Research
Restorative Medicine
Houston Methodist Advances Research into Neural Prosthetics
Noninvasive Spinal Stimulation Works to Restore Movement After Spinal Cord Injury
An Innovative Approach to Treat Even the Most Stubborn-to-Heal Fractures
Cell Encapsulation May Hold the Key to Preventing Cell Transplant Rejection
Houston Methodist, Rice University, Baylor College of Medicine Design Noninvasive Tech to Help Remove Brain’s Metabolic Waste
Houston Methodist Investigators Nanotechnology Investigators Awarded Prestigious Grants from the Department of Defense
Precision Medicine
Cancer Cell Type (Seed) and Tumor Microenvironment (Soil) Control Therapeutic Antibody Delivery and Efficacy
Novel Drug Combination Can Target Triple-Negative Breast Cancer for Treatment
A Houston Methodist and Purdue University Breakthrough May Result in a More Effective Tuberculosis Vaccine
Importance of the Coronary Artery Calcium Score in Risk Assessment and Prevention of Atherosclerotic Cardiovascular Disease
New Virtual Intensive Care Unit Simultaneously Improves Patient Care and Bed Capacity
result
Introduction
Joint Weill Cornell–Houston Methodist Academic Institute Doctoral Program Welcomes its Inaugural Class
Visionary EnMed Program Soars to New Heights
Neural Control of Organ Degeneration and Regeneration (NeuralCODR) Training Program
Faculty and Research Development
Graduate Medical Education


Science in Service
of
Medicineresult
President's letter
2021 Metrics
Cycle of Translation
Visionary Gifts of Hope
Introduction
Ann Kimball and John W. Johnson Center for Cellular Therapeutics at Houston Methodist
Houston Methodist Dr. Mary and Ron Neal Cancer Center
The Food & Health Alliance within the Houston Methodist Lynda K. and David M. Underwood Center for Digestive Disorders, Immunology Center and the Fondren Inflammation Collaborative
Houston Methodist Cockrell Center for Advanced Therapeutics
Paula and Joseph C. “Rusty” Walter III Translational Research Initiative
Jerold B. Katz Academy of Translational Research
Infectious Diseases Research Fund
From Discovery to Clinic
What is "Discovery to Clinic"?
Restorative Medicine
Houston Methodist Advances Research into Neural Prosthetics
Noninvasive Spinal Stimulation Works to Restore Movement After Spinal Cord Injury
An Innovative Approach to Treat Even the Most Stubborn-to-Heal Fractures
Cell Encapsulation May Hold the Key to Preventing Cell Transplant Rejection
Houston Methodist, Rice University, Baylor College of Medicine Design Noninvasive Tech to Help Remove Brain’s Metabolic Waste
Houston Methodist Investigators Nanotechnology Investigators Awarded Prestigious Grants from the Department of Defense
Precision Medicine
Cancer Cell Type (Seed) and Tumor Microenvironment (Soil) Control Therapeutic Antibody Delivery and Efficacy
New Virtual Intensive Care Unit Simultaneously Improves Patient Care and Bed Capacity
Novel Drug Combination Can Target Triple-Negative Breast Cancer for Treatment
A Houston Methodist and Purdue University Breakthrough May Result in a More Effective Tuberculosis Vaccine
Importance of the Coronary Artery Calcium Score in Risk Assessment and Prevention of Atherosclerotic Cardiovascular Disease
Translational Luminaries


Discovery to Clinic
Precision Medicine
Importance of the Coronary Artery Calcium Score in Risk Assessment and Prevention of Atherosclerotic Cardiovascular Disease
Importance of the Coronary Artery Calcium Score in Risk Assessment and Prevention of Atherosclerotic Cardiovascular Disease
Share this story



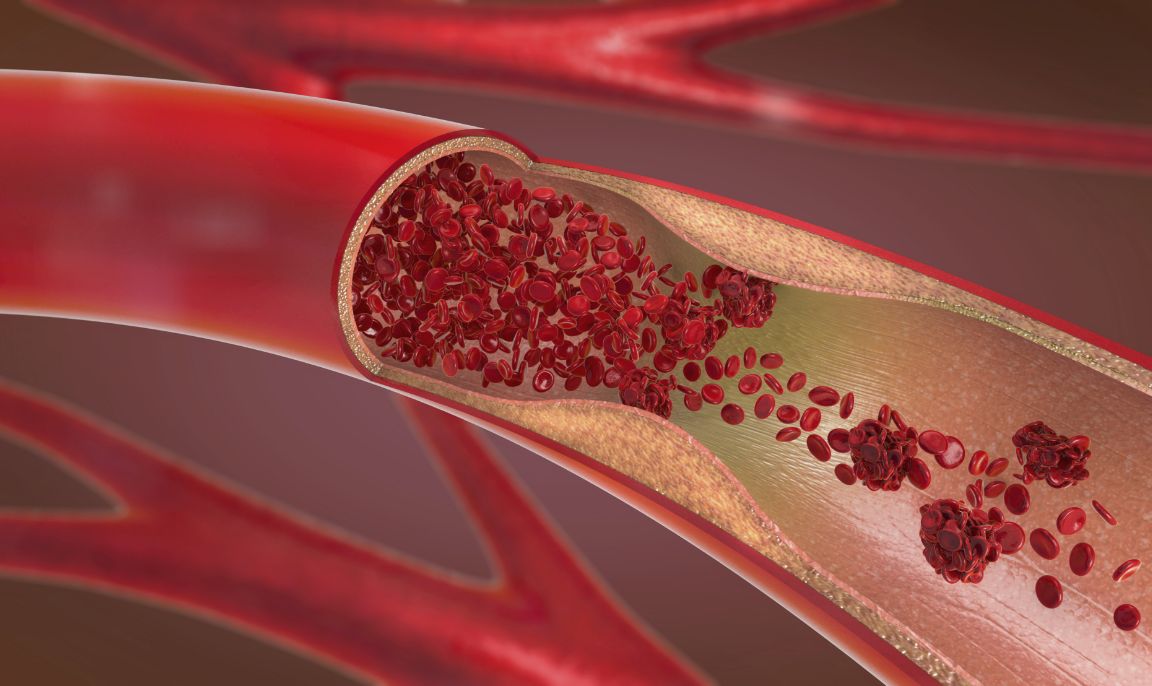
According to the Centers for Disease Control and Prevention (CDC), someone in the United States dies every 36 seconds from cardiovascular disease, making it the number one cause of death in the United States and a major cause of death globally. Atherosclerotic cardiovascular disease (ASCVD), which is caused by buildup of plaques in arterial walls, can potentially be prevented by the aid of the coronary artery calcium (CAC) score.
In general, it can be difficult to predict the presence of ASCVD. Traditional risk factors including age, weight, blood pressure and cholesterol levels suggest some risk, but they are insufficient in accurately predicting ASCVD risk in asymptomatic individuals. There is a great need for accurate estimation and prediction of ASCVD risk to minimize cost and misallocation of healthcare resources. In a recent review published in the British Medical Journal, Houston Methodist cardiologists Khurram Nasir, MD, MPH, the Jerold B. Katz Investigator and Professor of Cardiology, and Miguel Cainzos-Achirica, MD, PhD, MPH, assistant professor of preventive cardiology, discuss the history of the CAC score, key studies leading to its adoption in clinical practice guidelines and its role in the personalization of risk scoring and subsequent management strategies.
Using relatively inexpensive, low-radiation, non-contrast computed tomography scans, CAC scores can detect and quantify coronary atherosclerotic plaque. Today, more than 30 years after the inception of the score, there is ample support to continue using CAC as a decision aid when prescribing statins and potentially other preventive medications and interventions.
The CAC score offers critical insight for downstream decision-making and disease management strategies. Notably, that could mean refraining from or at least delaying expensive novel therapies, especially if the patient’s calcium score is zero.
Patients with a CAC count of zero have incredibly low rates of cardiovascular events during follow-up, or at least the lowest among their cohort. For instance, a 75-year-old patient with a score of zero does not have zero risk of cardiac events but is within the lowest risk category for their age and markedly lower risk than a 75-year-old with a high score. The same applies to patients with diabetes, severe hypercholesterolemia and other features that increase the average risk of cardiovascular events. How long that protection lasts is a subject of ongoing debate and research, although Nasir and Cainzos-Achirica recommend that patients with a CAC score of zero get their levels rechecked every three to five years.
Having a CAC of zero isn't just meaningful for the patient; it's empowering for the patient's physician as well. It allows for enhanced flexibility in terms of deciding which treatments and interventions are most appropriate to keep the patient on a healthy track. For example, if a patient in a traditionally high-risk category has a zero CAC score, you can have a nuanced discussion about taking a daily statin pill — based on lifestyle, interest, familial history, etc. — rather than just prescribing it. A similar reasoning applies to other interventions, with the added consideration of potentially large out-of-pocket costs.
Novel medications such as GLP1 receptor agonists for patients with diabetes or PSK9 inhibitors for patients with severe hypercholesterolemia can cost thousands per year, even with insurance. If the patient has an exceedingly high CAC score, the absolute reduction of risk can be dramatic with these interventions. But, if the patient has a CAC score of zero, the reduction in absolute risk will be more modest.
According to Nasir and Cainzos-Achirica, “In a context of progressively low estimated ASCVD risk thresholds for consideration of preventive therapy with statins in international primary prevention guidelines, CAC = 0, which is associated with low event rates in several populations, has become a particularly powerful prognostic tool and may be incorporated in clinician-patient discussions to guide the safe avoidance of preventive therapy with statins and aspirin. Moving forward, ongoing studies will help define the potential role of CAC informing the personalized allocation of other risk reduction therapies among several populations, such as individuals with diabetes and severe hypercholesterolemia.”
Studies conducted by Nasir, among others, suggest that patients are more compliant when they have an accurate picture of their burden of plaque. It improves adherence to both lifestyle changes and medication to know how much is riding on these interventions.


More from Discovery to Clinic


